Oakley Debbs was his parents’ pride, the 11-year-old from West Palm Beach, Florida was a straight A student with a sunny disposition and ready smile. Despite some struggles with asthma control, Oakley was an outstanding athlete – a gifted soccer and tennis player, flag football quarterback, and the marathon runner who scooped up the medals in all his races.
But tragically, his loving parents – Merrill and Robert Debbs – must now learn to speak of him in the past tense. While on a Thanksgiving vacation in Maine, Oakley ate some cake on Nov. 24, 2016 that contained either nut extract or nuts, and the boy with tree nut and peanut allergies suffered a fatal anaphylactic reaction.
As they prepare for a big memorial tribute to Oakley on Dec. 10, 2016 Merrill and Robert Debbs spoke to Allergic Living about their loss, their concerns about vital information they never got at the allergist’s office, and their resolve to raise anaphylaxis advocacy through their new Red Sneakers awareness campaign. (Red was Oakley’s favorite shoe color.)
“Whatever we can do to help people protect children who have these food allergies – labeling, education to protect these children so it never happens again,” says Robert of the couple’s decision to start a campaign and website while still coming to grips with their son’s death. Both parents now think they were far more informed about asthma than they were about the management of food allergies and risks of anaphylaxis.
While they were advised to avoid nuts and peanuts and knew some basics, “we have been in the hospital many times for asthma, so the nut wasn’t our real issue,” says Robert. “The focus had been 95 percent on controlling the asthma.”
To inform others, they relate what happened on that evening of Nov. 24. Their relatives had ordered a Thanksgiving gift basket with a ham, and it turned out to also contain items including a pound cake. “We didn’t even see the cake; it had just been opened up and set on the island of the kitchen,” says Merrill. But her son, who was normally very good about checking labels for nuts and peanuts, on this occasion just took a piece of cake when he could see no obvious sign of nuts. The trouble was, his father says, that Oakley hadn’t liked the food at a restaurant they had dined at and he was still hungry.
“He thought it was just a piece of cake,” says Robert. “But when he ate it, he came over and said it might have contained nuts.” His mother had some of the cake, and thought she tasted a nut flavor as well. “Merrill did what we usually do, she gave him Benadryl [pills],” says Robert. “And he came back and he said that he felt fine.” His only symptom, at that point, was a hive on his lip, which went away with the antihistamine.
But that would soon change. Oakley and his mom went upstairs to get ready for bed. They brushed their teeth together, and he mentioned having some pain in his chest, “just a little soreness on the left side,” says Merrill, who notes that at that point “he was breathing fine.” They turned in for the evening, he in a room with his cousins, she in a room a floor above. About 15 minutes later, Oakley came up to his parents’ room, complaining of a stomach ache. Suddenly, he needed to vomit.
He felt better afterward and Merrill put him in bed with her, giving him more Benadryl (he’d thrown up his pills). Quite soon, he needed to be sick again. Back in bed, his mother set up the asthma nebulizer, since her son’s breathing was deteriorating, with her mother-in-law now in the room trying to help. Merrill was about to give her son prednisone when he suddenly blurted out to call 911.
With both her mother-in-law and husband now in the room, Merrill ran to do just that. Although the EMTs arrived swiftly, Oakley’s blood pressure had dropped and he suffered a heart attack and fell unconscious. The EMTs gave the boy two successive doses of epinephrine, but this was well over an hour after he’d eaten the cake. Oakley later died in hospital from this severe reaction.
In hindsight, the Debbs feel they were not adequately informed of the risks of food allergies by their allergist’s office. While they own an epinephrine auto-injector, the couple say they weren’t aware that it is the only first-line drug for anaphylaxis (since antihistamines can’t stop systemic symptoms). “I wasn’t aware, no one told me,” says Merrill.
“So our advocacy also relates to the fact that we didn’t know that,” says Robert, explaining his sense that far greater education and communication between allergists and their patients is needed.
Nor had the Debbs been made aware of the Natalie Giorgi case and newer allergists’ advice since her passing in 2013 to err on the side of using epinephrine if a known food allergen is consumed.
Both parents say that their son had numerous allergy triggers – from pollens, to cats, birds, feathers and dust mites. And he’d also tested positive to nuts and peanuts. But Merrill says that other than strict avoidance, they weren’t given much information about food allergy management. “I knew the asthma, and I treated him for asthma every day.”
Of her hopes and ambitions for the Red Sneakers campaign in the months ahead, Merrill comments on the need to channel Oakley’s tragedy into something positive for her family, which includes the boy’s twin sister, and for the food allergy community as a whole.
“This child of mine, he was a rock star, he was a good, good kid. And always in my heart of hearts, I knew that he would make a difference in his life – I just didn’t know it would be after he passed away. So that’s a big part of my driving force – the legacy of Oakley.”
For those who live with a life-threatening allergy, an EpiPen is an essential item to keep on hand. EpiPens contain a single dose of epinephrine, which works quickly to combat the life-threatening symptoms of anaphylaxis. Epinephrine works rapidly to stimulate the heart, improve breathing, reverse hives, raise dropping blood pressure, and reduce swelling in the throat, lips, and face.
There are many brands of epinephrine injectors, but most people have seen images for the EpiPen with the blue safety cap and orange tip that contains the needle. However, there is a new innovative product called the Auvi-Q, which is shaped like a smartphone and gives automated verbal instructions to lead a person through the injection. Check out the images of each below:
Here are five things every patient or caregiver should know about using an EpiPen:
How to handle it. You should always be sure to take off the safety cap and hold the pen with your fingers around it in a fist. Do not put your thumb on top of the EpiPen. Different brands of this medication have varying instructions for preparing and using the injector. Be sure to learn to properly handle and inject the medication in advance so you will be prepared to use it when the time comes.
Where to inject it. The epinephrine should be injected directly into your outer thigh. It should not be injected into your hands, fingers, feet, buttock, vein, or any other part of your body. Seek immediate medical attention in the case of an accidental injection.
It can be administered while wearing pants. Contrary to popular belief, the EpiPen injection can be delivered through clothing.
Count to 10 while administering the epinephrine. After you inject it into your thigh, hold the EpiPen in place and count to 10. This will allow the medication enough time to be delivered into your body.
When you give or take the injection, call 911 immediately. Epinephrine is fast acting, but temporary. After giving or taking an injection, you should immediately seek medical treatment, even if you are feeling better. Tell the medical professional that you have injected epinephrine.
Allergens produce a wide range of symptoms. Some allergens cause mild inconveniences, like hay fever, and other allergens, such as bee stings or peanuts, can produce deadly reactions. Experts estimate that around 5 percent of the population has an insect allergy and around six million children in the U.S. are allergic to at least one food. There’s no telling how an allergic reaction will manifest. Allergic reactions can include hives, swelling and even anaphylactic shock. Even if someone has never had a severe reaction before, they still may be susceptible to one. Because of this, many experts agree that all people with known allergies should carry an EpiPen for safety.
How Does an EpiPen Work?
EpiPens are auto-injectors that deliver a dose of epinephrine to someone who is having an allergic reaction. The medication inside opens up airways and narrows the blood vessels. It can help stop serious symptoms like wheezing, severe skin itching, tightening of the throat and low blood pressure.
EpiPens can be used to treat severe allergic reactions that are caused by food, medications, latex, insect bites or stings and exposure to other allergens.
How to Use an EpiPen
The EpiPen can be used by the person who is having the allergic reaction. There is a safety cap that must be removed before using the EpiPen. It works by making an injection into the muscle of the thigh. If you have never used an EpiPen, you should ask your doctor about getting a trainer pen so you can get used to using the device.
The effects of the EpiPen are not long-lasting. In many cases, the effects wear off after about 20 minutes. If necessary, you can do an additional injection with the EpiPen while you are waiting to receive further medical care.
Even if someone is doing better after treatment with an EpiPen, it is still important to get them to an emergency room as soon as possible. The allergic reaction may come back if they do not receive treatment right away. The doctor may wish to do another epinephrine treatment; however, it is not advised that people do more than two treatments without the supervision of a doctor.
Who Should Carry an EpiPen?
Anyone who has had a severe allergic reaction at any time in his or her life should carry an EpiPen. EpiPens should also be carried by the parents of young children who have been diagnosed with an allergy. Allergens that are most likely to have severe effects include peanuts, shellfish, latex and insect stings.
EpiPens are available by prescription and usually covered by insurance. While you may never need one, having one can help avoid serious anaphylaxis and even save a life.
There are some people who should not use EpiPens because of health risks. EpiPens are not recommended for people who have conditions such as:
Diabetes
Thyroid disorders
A heart rhythm disorder
Coronary artery disease
High blood pressure
Heart disease
Parkinson’s disease
People who have or develop any of these conditions should talk to their doctors about whether EpiPens are safe and what alternatives are available.
Emily, my 11 year- old sister, has a severe peanut and tree nut allergy. Some children grow out of their allergy, but in Emily’s case, it is different. She has a life threatening allergy which gets worse as she grows older. In order to keep her safe, she carries around an epinephrine (Epi) pen. She uses an EpiPen in case she comes in contact with a peanut or even a food with a trace of peanut.
At the age of two, Emily found out she was allergic to peanuts. Her Grandpa gave her a handful of chopped nuts at a buffet and Emily immediately, started to develop hives on her face, especially around her mouth. She told her mother that her ears itched and her tongue hurt. Her tongue had already started to swell.
Emily was immediately taken home and administered Benadryl. She was referred to Dr. Ray S. Davis, a child allergy and asthma specialist with Allergy Consultants in St. Louis, MO. Dr. Davis prescribed an EpiPen, which contains a prescription drug. Thankfully, Emily has never had to use the EpiPen.
According to the National Institute of Allergy and Infectious Diseases, 11 million Americans suffer from food allergies, and 100 to 200 of them, mostly children, die each year from allergic reactions.
According to WebMD, a peanut allergy is a reaction that occurs when your body mistakenly identifies peanuts as harmful substances. When you eat peanuts or food containing peanuts, your immune system—the body’s natural defense system that fights infections and diseases—overreacts and can cause a serious, even life-threatening response called anaphylaxis.
WebMD states that there are many foods people are allergic to, but the main foods are: peanuts, tree nuts, dairy, eggs, fish and shellfish. People can also be allergic to stinging insects, medications and latex.
The Allergy and Asthma Network states that anaphylaxis is a sudden severe allergic reaction that may affect the whole body. Symptoms can include hives, swelling of the lips, throat or tongue, vomiting, shortness of breath, wheezing and coughing. In more severe cases, a drop in blood pressure or a loss of consciousness may occur. Symptoms can develop within seconds after exposure to the allergen.
An EpiPen is required for individuals who have food allergies and is a treatment for anaphylaxis. The EpiPen is an adrenaline hormone that increases your heart rate and blood pressure and reverses the swelling of the airways.
According to WedMD, the EpiPen is injected anywhere between the person’s hip and knee because the epinephrine is readily absorbed intramuscularly. It should never be injected into a vein, since this would cause an unsafe increase in blood pressure and possibly cause bleeding. The effects of an EpiPen only last 15 to 20 minutes. Therefore, 911 should still be called immediately. In some cases a second dose is required.
“I try the best I can to keep my child safe,” says Karen Meara, a nurse and Emily’s mom. “When I go to the grocery store, I have to read the ingredients on everything. Every time we go out to eat, I ask the chef for a peanut free menu, which lists the foods that are okay for my child to eat. It is very challenging traveling, especially out of the country, or going to places where there are no labels to read. Another challenge with a child that has a peanut allergy that most people would not think of is buying safe toiletries. Many products such as shampoo, conditioner, soaps, and lotions contain coconut or almond oils. These products have not been thoroughly tested, so I avoid them.”
“I have the option of sitting at a peanut free table [at school],” says Emily. “I get to sit with friends, but they also know to bring peanut-free lunches.”
Congress has approved a bill in 2004, called the Food Allergy Labeling and Consumer Protection Act, that is designed to help people with food allergies. This bill has required food manufacturers to make food labels easier to read and include if the product is manufactures in the same facility as other food allergens. According to Stefano Lucciolo, M.D., senior medical advisor in the Food and Drug Administration’s Office of Food Additive Safety, there is no cure for food allergies and this law helps protect citizens.
People who have peanut/tree nut allergies need to avoid the obvious foods, such as nuts and peanut butter. In addition, there are foods that contain nuts or have been manufactured in a facility that processes nut products. Here are some examples. Credit: Kaitlyn Meara.
It is not uncommon for a school’s health office to be filled with several EpiPen’s. Schools also have to deal with a new form of bullying which entails students wiping peanut butter on children with peanut allergies. Davis warns his patients about this, and instructs the parents to make sure several EpiPen’s are readily on hand at school.
Emily states,”It makes me feel good knowing I carry an EpiPen because it will help me breathe in case I accidentally eat a peanut,” states Emily. “The EpiPen gives the ambulance enough time to get there. Even if I grow out of my peanut allergy, I would still never eat a peanut because the tests may be wrong and I don’t want to take any risks. It has affected me because when I go to birthday parties, I am not allowed to eat cake or any of the other treats, especially those without a label.”
As for me, I am very protective of my younger sister and am constantly looking out for her safety. I am also proficient in the proper use of an EpiPen. Kaitlyn Meara
Did you know that tree nuts are one of the most common food allergens in Canada? For people who are allergic, avoiding tree nuts and foods that contain tree nuts while still eating a healthy diet is important. Read on to get the facts on tree nut allergies.
What is a tree nut allergy?
A tree nut allergy is when the body’s immune system mistakes tree nuts as harmful. For some, tree nuts can trigger life-threatening reactions.
What are tree nuts?
Tree nuts include:
Almonds
Brazil nuts
Cashews
Hazelnuts
Macadamia nuts
Pecans
Pine nuts
Pistachio nuts
Walnuts
Peanuts are legumes and are not considered a tree nut. Learn more about peanut allergies here.
What are the symptoms of a food allergy?
Like other food allergies, having an allergic reaction to tree nuts can include any of the following symptoms:
Flushed face, hives or a rash, red and itchy skin
Swelling of the eyes, face, lips, throat and tongue
Trouble breathing, speaking or swallowing
Itchy skin
Anxiety, distress, fainting, paleness, sense of doom and weakness
Cramps, diarrhea, vomiting
A drop in blood pressure, rapid heartbeat and loss of consciousness (in extreme cases)
When is a tree nut allergy usually diagnosed?
Treat nut allergies can be diagnosed in childhood and adulthood. However, they are most often diagnosed in early childhood.
If I am concerned about tree nut allergies, should I delay feeding it to my infant?
No. There is not enough evidence to say that avoiding tree nuts will lower the risk of an allergy. However, avoid whole nuts and chunky nut butters because they are choking hazards. Try smooth nut butters like almond or cashew, spread thinly on toast or crackers instead. Speak with your doctor if you have a concern about introducing specific foods to your infant.
Can a tree nut allergy be outgrown?
Not likely. Tree nut allergies in children are less likely to be outgrown compared to other common food allergies.
What foods may contain tree nuts?
Foods and drinks that often contain tree nuts include:
Asian dishes like pad thai or chicken satay
marzipan
tree nut oils
pralines
spreads, like almond-paste spreads, cheese spreads and chocolate nut spreads
vegetarian dishes
Food products that possibly add tree nuts include:
baked goods
baking mixes, cereals, crackers and muesli
barbeque and pesto sauces
dressings and gravies
flavoured coffees
frozen desserts
liqueurs like amaretto
natural flavourings and extracts, like almond extract
salads
snack foods like trail mix
What are other names for tree nuts?
Tree nuts can have many other names including:
anacardium nuts
hazelnuts (filberts)
nut meats
pinon
macadamia (queensland nut)
Stricter Canadian guidelines require foods that have tree nuts to be clearly labelled. The ingredient list will say “contains: almonds, Brazil nuts, cashews, hazelnuts, macadamia nuts, pecans, pine nuts, pistachios or walnuts” if it contains these tree nuts.
Is it safe to eat peanuts if you have a tree nut allergy?
It can be. If you are only allergic to tree nuts, you can eat peanuts. However, some peanuts are cross contaminated with tree nuts when they are processed and manufactured. Consult with your doctor or allergist before consuming peanuts as part of your regular diet.
Tips for following a tree nut free diet
Keep these helpful tips in mind when following a tree nut-free diet:
Look for the words “contains: almonds, Brazil nuts, cashews, hazelnuts, macadamia nuts, pecans, pine nuts, pistachios or walnuts” on the ingredient list. All tree nut-containing foods are now clearly labelled.
Read the label every time. Food manufacturers often change ingredients used in their products without notice.
Avoid food product labels that say “may contain” or “may contain traces” of tree nuts on their label.
If you are unsure if a product contains tree nuts, contact the manufacturer. Many food packages have contact information on them.
Don’t take chances. Avoid foods that do not have a clear ingredient list. This includes avoiding imported products, as they do not always have an accurate food label.
When eating out, ask if dishes have been prepared using tree nuts. If you can, call ahead to see if nut-free dishes are available.
Instead of adding nuts to baking, try rolled oats, dried fruit or rice cereal for a satisfying texture.
Looking for a mid-day snack that’s nut free? Try snacking on homemade granola on its own or add it to yogurt.
Bottom line
You can still eat a healthy balanced diet following Canada’s Food Guide if you have a tree nut allergy. If you aren’t sure if a product contains tree nuts, don’t take any chances. Carefully reading the ingredient list of food products every time is important to avoid an allergic reaction.
AAFA supports school policies that promote access to life-saving medications to treat students and staff who experience severe allergic reactions. States should implement policies that promote access, including supplying schools with epinephrine auto-injectors to be used in emergencies, appropriately training school personnel and addressing liability concerns for those who use this medication in good faith.
Food allergies continue to be a growing problem, especially among young children. Approximately 15 million people in the United States suffer from food allergies, 6 million of whom are children. These children spend much of their day in school, where they may be exposed to food allergens which can trigger a severe immune response, known as anaphylaxis.
AAFA urges state legislators to make the simple decision to save young lives. If schools have access to undesignated epinephrine auto-injectors and staff trained to administer the medication, we can avoid tragedies in the classroom.
Expanding Access to Epinephrine Beyond School Campuses
As the number of states allowing schools to maintain an emergency supply of epinephrine auto-injectors increases, many states are looking beyond the classroom to other areas where food allergy triggers could be present. In any public space where food is present – such as sports and recreation venues, summer camps, amusement parks, movie theaters – there is a risk for an allergic individual to come in contact with their allergen. Therefore, focus is widening to consider epinephrine stocking laws beyond schools and into other public “entities.”
View the map below to learn about the status of entity epinephrine stocking in your state.
To learn more about entity stocking laws, please see the featured Spotlight Article in AAFA’s 2015 State Honor Roll™ Report.
Does Your State Stock Epinephrine in Schools?
The School Access to Emergency Epinephrine Act
In 2013, President Obama signed the School Access to Emergency Epinephrine Act into law. This federal law encourages states to implement policies requiring schools to stock undesignated epinephrine auto-injectors for use in emergencies. States who develop such policies will be given additional preference for federal grants.
While this law sends a strong message from the federal government about the importance of being prepared to treat anaphylaxis, we still need to work to ensure that all states pass epinephrine stocking laws for schools!
(Reuters Health) – If restaurants and other food establishments stocked epinephrine autoinjectors, the number of fatal allergic reactions, known as anaphylaxis, could decrease, a small study in Canada suggests.
After a two-year test of an epinephrine autoinjector stocking program in Hamilton, Ontario, diners with allergies as well as restaurant owners and staff said that having the devices onsite made them feel better about possible emergencies, researchers report in The Journal of Allergy and Clinical Immunology: In Practice.
The costs varied by how many staff needed to be trained to use the devices, but the expense was low compared with that of automated external defibrillator (AED) devices, the study authors note.
“Self-management of food allergy and anaphylaxis is sub-optimal, particularly among adolescents and young adults who most often engage in risk-taking behaviors such as neglecting to carry epinephrine autoinjectors or delaying its timely administration to treat reactions,” said lead author Dr. Susan Waserman, a professor of medicine at McMaster University in Hamilton and director of the Adverse Reactions Clinic at the Firestone Institute of Respiratory Health.
Between 1986 and 2011, about half of anaphylaxis deaths in Ontario were due to food allergies, and 14 percent occurred after eating at restaurants, fast food chains or shopping mall food courts.
In the U.S., more than half of anaphylaxis deaths occur at restaurants or other food establishments such as ice cream shops and food courts, the study team writes.
“Challenges also exist in food establishments, including the lack of knowledge and training of food service personnel about food allergies and the reluctance of food-allergic individuals to disclose their allergies to restaurant staff due to embarrassment,” Waserman told Reuters Health by email.
To test the feasibility of stocking epinephrine injectors in places where severe allergic reactions to food might occur, the researchers implemented a program at a Hamilton shopping mall between 2014 and 2016. Security guards had access to autoinjectors in first aid kits in the mall’s central administration office and received training on recognizing allergic reactions and how to use the injectors.
In two mall restaurants, staff were also given the three-hour training session and had access to injectors kept in a central area, such as behind the counter, as well as back-up doses kept in an office area. Each location also had a site leader and an anaphylaxis emergency response plan.
Only one critical incident occurred during the study period, so it is difficult to show the full benefits of the program, the study team writes.
However, since the pilot program, government-owned properties in Hamilton such as recreation centers, arenas, senior centers and community halls have installed autoinjectors. After finding that firefighters often arrive on the scene for anaphylaxis emergencies before ambulances, the Hamilton Fire Department also stocked its fire trucks with autoinjectors. The program is now in 50 restaurants across the city, with the goal of reaching all 2,000 restaurants in Hamilton.
The success of the epinephrine autoinjector stocking program depends on several factors, including local government support, effective staff training, low resource requirements and embedding the program into existing policies and procedures, Waserman’s team writes.
Costs in the pilot program ranged from C$715 ($543.93) for the sit-down restaurants to C$2,155 ($1,639.41) for the mall-wide program, they note.
“Whether you’re diagnosed with an allergen already or have your first allergic reaction at a restaurant, this could stop a potentially life-threatening moment,” said Dr. Scott Sicherer of the Icahn School of Medicine at Mount Sinai in New York City, who was not involved in the study.
“When you eat outside of your home, you depend on other people to make food for you,” he said in a phone interview. “This program is a good model that makes sense.”
Legislation and liability issues may pose more of a problem in the U.S., he added, since epinephrine autoinjectors are typically only available by prescription. Now that some schools are beginning to carry them, however, that could open the door for other public places.
“At a restaurant, you can say you have an allergy and you can carry a card with instructions,” Sicherer said. “A chef or server may guarantee they can provide a safe meal, but when that means just scraping nuts off the top of a salad, that doesn’t work, and you may not realize.”
SOURCE: bit.ly/2nEwQIWThe Journal of Allergy and Clinical Immunology: In Practice, online August 2, 2018.
12-year-old Kennedy Pelletier is no stranger to food allergies having discovered she was allergic to fish and shellfish after suffering a reaction at Disney years ago. She had a subsequent reaction at a restaurant in 2018 despite avoiding her allergens when her dish was likely contaminated due to cross-contact.
The seventh-grader decided it was time for action to protect others who might suffer reactions while dining. She contacted State Senator Jim Welch, urging him to sponsor a bill that would allow restaurants to carry stock epinephrine. Epinephrine is the only drug that can halt the progression of anaphylaxis, a severe, life-threatening allergic reaction. Stock refers to doses of the drug that are not prescribed to any individual and may be administered in an emergency.
Kennedy’s class traveled to the Massachusettes statehouse Tuesday to testify before the Joint Committee on Public Health on Welch’s bill, S.1355. The bill would allow an individual suffering an allergic reaction, a family member, or healthcare provider to administer the restaurant’s supply of the drug in an emergency while shielding the restaurant and participants from liability.
“We share her concern that many people who have life-threatening allergies don’t know they have life-threatening allergies before they have a severe reaction,” said Kennedy’s mother, Michelle Regnier-Pelletier.
Though the legislation does not require restaurants to carry stock epinephrine, Sen Welch intimated his goal is to eventually mandate that all restaurants carry.
“I think a restaurant can bear the cost of one EpiPen for the safety of all their customers,” Welch said.
With the summer winding down and the academic year in full swing, school-age severe allergy sufferers have to cope with more than just purchasing requisite school supplies and cool-weather gear. They should also be sure to have their emergency epinephrine treatment on hand and ready for use, particularly in light of its seemingly scarce availability. The Pfizer/Mylan supply shortage of brand and generic EpiPen and EpiPen Jr that was first announced in 2018 is ongoing as of September 2019, with no end in sight.
“EpiPens, especially at the beginning of school years, can be difficult to find for patients,” said Ryan Israelsen, MD, a board-certified allergist and immunologist from the Allergy and Asthma Center of Southern Oregon. “If they can’t find an EpiPen at their pharmacy, [they should] ask if there’s a generic available,” he said.
Yet, the shortage has affected both the Pfizer EpiPen and its generic alternative from Mylan.
“We share in the frustration over the fluctuating availability, but, as with many sterile injectable medicines, EpiPen requires a highly complex and technical manufacturing and assembly process,” said Pfizer spokesperson Kim Bencker. “Despite our significant efforts, we do anticipate further supply shortages over the coming months,” she said, adding, “We are committed to resolving this availability issue as quickly as possible.”
Alternatives unaffected by shortages
Kaléo, which manufactures a competitor auto-injector, Auvi-Q, has no such availability concerns. “Kaléo has not been impacted by the supply issues reported by other epinephrine auto-injector manufacturers,” said Caryn Foster Durham, director of corporate communications at Kaléo.
Kaléo partnered with Walgreens in 2018 to offer its 0.15-mg and 0.3-mg products—corresponding to the EpiPen Jr and EpiPen doses, respectively—either at no cost or via a patient assistance program. A newly approved 0.1-mg dose, the first specifically designed for use in infants and toddlers, is also included in the Walgreens collaboration.
Whether Auvi-Q use or sales have increased due to the EpiPen shortage is unknown, however. “Kaléo does not share specific sales information related to our products,” said Durham.
Symjepi, another contender in the field of emergency epinephrine delivery systems, also has 0.15-mg and 0.3-mg doses currently available. Symjepi is a prefilled syringe and device combination rather than an auto-injector, but its size and ease of use make it a viable alternative, said Allison Schneider, director of communications at Sandoz, which markets Symjepi.
“It’s small … has an intuitive, user-friendly design, a smaller needle than the auto-injectors, and fits into the palm of your hand,” she said. Symjepi, which has been available in retail pharmacies since July 2019, also has a savings program that allows eligible patients to obtain it at no cost, Schneider noted.
Are beyond-expiration date products safe to use?
Patients who prefer the EpiPen brand or its generic alternative can safely use many lots of these products for 4 months beyond their expiration dates, according to research findings on their stability, Pfizer announced in a 2018 statement. Since then, Amneal, which manufactures generic EpiPen and EpiPen Jr, provided data to support the use of specific lots of both products for 2 months beyond their listed expiration dates.1
Israelsen agrees that when a patient’s preferred product is unavailable, “they can carry an old epinephrine auto-injector, and if there’s no crystallization or ‘floaties,’ it’s safer to use than nothing.” For new patients, however, “I try to show them the options and let them choose,” he said.
Kari Trotter Wall, PharmD, a director of pharmacy at both University of Southern California (USC) Pharmacy and USC Health Center Pharmacy in Los Angeles, generally recommends against using expired products.
“I don’t usually advise people [to use] past expiration dates because I like to do whatever I can to get the product for them,” Wall said. She described how staff at her pharmacies, which mainly serve college students, faculty, and staff, will call around if a prescribed product is unavailable at their location.
“The priority is that [patients] get something in hand,” she said. “Ideally I would like it to be from me, but if I don’t have it, I’m going to try to get it.”
What federal laws protect people with asthma and allergies?
The following are key laws that protect people with asthma and allergies in the US.
CDC Public Health Law for Asthma
School Access to Epinephrine Emergency Act
This law amends the Public Health Service Act to increase the preference given, in awarding certain asthma-related grants, to certain States (those allowing trained school personnel to administer epinephrine and meeting other related requirements).
Section 504 of the Rehabilitation Act of 1973
This law is commonly referred to in the school setting and defines a person with a disability as someone who has an impairment (either physical or mental) that substantially limits major life activities (such as eating and breathing and going to school), or who is regarded as having such impairments.
This law prohibits discrimination on the basis of disability and can support families in pursuing appropriate accommodations as needed.
Food Allergen Labeling and Consumer Protection Act of 2004
FALCPA is an amendment to the Federal Food, Drug, and Cosmetic Act and requires that the label of a food that contains an ingredient that is or contains protein from a “major food allergen ” declare the presence of the allergen in the manner described by the law.
What state laws protect people with asthma and allergies?
States have enacted laws that protect people with asthma and allergies. The three laws most relevant to those with asthma and allergies are:
Student rights to self-carry epinephrine and albuterol inhalers
School epinephrine and albuterol stocking
Entity/public place stock epinephrine
Student rights to self-carry epinephrine and albuterol inhalers
All 50 states now have laws protecting students’ rights to carry and use prescribed asthma and anaphylaxis medications.
Why is it important to allow students the right to self-carry their asthma and anaphylaxis medications?
Every school year students have died because they were unable to get to their asthma or anaphylaxis medications on time. The medications were locked in a nurse’s cabinet or stowed away in a place too far to get to when the student needed them. Minutes count when asthma or anaphylaxis strikes. Students need to carry these medications on them, know when and how to use them — and then do it.
What if my child’s school doesn’t allow my child to self-carry asthma and anaphylaxis medications?
Parents, teachers, school nurses — contact local schools and make sure they know these laws exist and what they mean. If you need the text of the law for your state, please contact us.
What was the Network’s role in passing these self-carry laws?
We spearheaded a Breathe: It’s the Law is an awareness campaign to make sure students in every state had the right to carry and self-administer their life-saving asthma and anaphylaxis medications. We played worked with volunteers and legislators in every state to get these laws passed in all 50 states.
In 2002, Allergy & Asthma Network held an Allergy & Asthma Day Capitol Hill briefing about the plight of schoolchildren whose asthma medications were locked in the clinic instead of by their side at all time as prescribed by their physicians. Tragically, each school year there were reports of students who did not receive medication in time. They died. The same was true of students with anaphylaxis and their access to prescribed epinephrine auto-injectors.
As a result of those hearings, members of Congress joined with Allergy & Asthma Network and advocates across the country to pass the “Asthmatic Schoolchildren’s Treatment and Health Management Act of 2004” (H.R. 2023). Signed into law in October 2004, this groundbreaking legislation gave funding preference to states that protect student’s rights to carry and self-administer asthma and anaphylaxis medications at school.
School stock albuterol and asthma management
A number of states across the country have passed laws or guidelines that permit schools to stock albuterol with a prescription and administer it to a student believed to be in respiratory distress and standardize asthma action plans.
This type of preparation and management in schools will not only improve a child’s health, but will also ensure students are able to focus on learning.
Currently 14 states have laws or guidelines to implement asthma action plans and increase access to appropriate and timely asthma treatment for students while in school. Action at the federal level is pending in the 116th Congress. The “School-Based Allergies and Asthma Management Program Act” (H.R.2468) was introduced by House Majority Leader Steny Hoyer (MD) and Rep. Phil Roe (TN) in May 2019 and incentivizes states to act.
Check the status of your state in the map below. States colored light blue do not have stock albuterol legislation.
Why is it important for schools to stock albuterol?
Stock albuterol laws across the country help save the lives of students who experience an asthma attack at school and do not have a prescribed albuterol inhaler with them.
School Stock Epinephrine Laws
All states now have laws that allow or require anaphylaxis emergency preparedness plans that permit schools to stock emergency supplies of epinephrine auto-injectors.
Why is it important for schools to stock epinephrine?
Stock epinephrine laws across the country help save the lives of students who experience anaphylaxis at school and do not have a prescribed epinephrine auto-injector. Access at school is critical because 25 percent of anaphylaxis reactions at school occur in students previously undiagnosed with a severe allergy to food, insect venom, latex or medication.
The stock epinephrine in schools law was often the first of its kind to deal with stocking non-patient specific emergency medications in the school setting. They have since been used as a template or foundation for other emergency medications.
What can I do if my child’s school does not stock epinephrine?
If your state has a law, there could be issues with implementing the law at your child’s school.
If there is not an existing state law, there is still work to be done in statehouses, legislatures and schools as lawmakers and policy makers develop law and implementation policies.
Please contact us for a copy of the law for your state or to find out how you can get involved with improving school access to stock epinephrine in your state.
Entity/public place stock epinephrine
Stock epinephrine has now moved beyond the school walls and out to public venues – from theme parks, restaurants and sports arenas to daycare centers and more. Many states passed entity epinephrine laws that permit public venues to stock emergency supplies of epinephrine auto-injectors.
Why is it important for entities and public places to stock epinephrine?
These laws allow restaurants, theme parks and other public entities to respond to a life-threatening allergic reaction in the event someone experiences anaphylaxis and does not have an epinephrine injector with them.
All too often these days, we read about another life lost to food allergies – generally in our younger community. Personally, I can’t imagine how I would react if it were my child. Would I struggle to live normally during a lifelong grieving process?
Would I avoid talking about what happened to my child and food allergies in general? Or would I have the courage, strength, and drive to dive deeper into the food allergy world in an effort to save others from facing similar devastation?
The past few years have seen greatness arise from such tragedies. Consider Red Sneakers for Oakley or Project Abbie. Years prior, however, the food allergy world gained a new superhero, driven to his mission by his son’s early passing from a peanut. He has shared his story many times over the past decade, raised hundreds of thousands of dollars for food allergy research, and is still motivated to do more.
His name is Brian Hom and you need to read his story.
There are some very important lessons that should cause some of us to take pause and reconsider how we protect ourselves or those we love. I am so grateful for Brian’s willingness to share his story with me for the benefit of all of us. I can’t imagine it’s ever easy.
Paul Antico: Brian, thank you for taking the time to speak with me today. A significant part of your life over the past decade has been impacted by food allergies and food allergy advocacy. Would you mind sharing the details of your story?
Brian Hom: This all began on July 1, 2008 when my family planned a special vacation to Cabo San Lucas, Mexico for my son who had just graduated from high school and celebrated his 18th birthday on June 25.
Early that morning, my wife, my three sons, and I left our home to fly down to Cabo. We arrived in Cabo around 6:00 or 7:00 at night and got to the resort around 8:00 pm. The restaurants were about to close so we just threw our suitcases in the room and went to eat at one of the restaurants in the resort. Everything seemed fine; it was a nice dinner. Later, we strolled along the beach to take a look at the facilities.
I came upon an arcade where I hung out with my three sons. Then my oldest son, B.J., who was 18 and had a peanut allergy, came to me and said, “Dad, my throat hurts. Can we go get some cough drops?” We went to the gift shop, got some cough drops and he walked away with my wife to continue touring the facilities while I was with my two other sons at the arcade. A lady who was on the airport shuttle bus with us then came to me and said, “You need to go to the lobby, your son’s fallen ill.” I’m thinking, “This is summertime, he’s healthy, now what’s going on?”
When I got to him in the lobby, his lips were blue, his face was pale, and I thought he was choking on the cough drops. He couldn’t talk; he was gasping for air. My first thought was, “Where’s the doctor?” They were supposed to have a doctor at the facility and there was no doctor. They said he had left at 5:00 and I asked, “Is there an ambulance available?” They said they were calling one. The staff at the resort started to do CPR on my son because he had basically gone unconscious.
It seemed like forever for the ambulance to get there, but it finally arrived and the paramedics tried CPR. My son was just getting colder and colder – his body was getting colder and my wife was holding him. The doctor finally got there and he took a pulse on his neck, put his head up to my son’s lips and just turned to me and said, “Sorry,” and covered him up with a sheet. He had passed away.
I didn’t know what to think about it, until I noticed that my younger son, Steven, who was 13 at the time, had a runny nose and was getting itchy and stuff. So, my first thought was, “Maybe there was something in the food.” I went to the resort management and I said, “Can you check with the chef to see what was in the food?”
We found out that there were traces of peanuts in the chocolate mousse that triggered the anaphylaxis in my son B.J. who had never suffered anaphylactic shock in his 18 years. He had his first incident, a peanut allergy reaction, when he was two years old and the doctors prescribed him an EpiPen at that time. But the next year it expired, and we’d go for annual checkups with the doctors, who never really focused on his food allergy. He was born in 1990 and, back then, food allergies weren’t very prevalent.
Paul Antico: I’m so saddened to hear this story and so sorry about the loss of your son. In the 18 years he had a peanut allergy, did he ever have other reactions?
Brian Hom: Yes, he would a get rash, itchy throat, maybe a runny nose. His eyes would get kind of red, but never did it cause him a problem breathing or closing of the throat. In Mexico, when he had that anaphylactic reaction, there was no rash, there was no itchy throat, nothing other than that his throat was closing on him. There were no signs of his normal symptoms when he eats something that he was allergic to, like the peanut, where he would basically start getting itchy—he would start scratching, he would get hives. But none of those symptoms came along.
Paul Antico: Roughly how many times had B.J. had peanut exposures and these lesser reactions, prior to this anaphylactic event?
Brian Hom: I’d say around 10, maybe.
Paul Antico: Okay, because I see two incredibly important takeaways that I’d love to just get your comments on. One is that the medical community always tells us—and again, it’s very different now than it was in 2008, for sure—to understand that the severity of one reaction doesn’t imply the severity of future reactions. Frankly, even I’ve had a hard time grasping that with two of my kids’ allergies, where the reactions have always been modest. Though your story is a huge wake-up call for me and, I’m sure, many others.
The second takeaway is obviously that we should always carry epinephrine, even if prior reactions have been mild.
I assume you agree with these, but I’m wondering if you had any other thoughts on them.
Brian Hom: Oh, definitely, I agree.
Yes, at my restaurant [which we discuss a little further down], I talk to hundreds, if not thousands, of people that say, “I only get mild reactions. I know, my tests show that I should have severe reactions but I don’t, and so I don’t carry an EpiPen.” My warning to them is, all it takes is one bad reaction, and if you can’t get to the emergency room quickly, it could be fatal.
My third son, who has a peanut allergy as severe as my son B.J., who passed away, had his first anaphylactic reaction at 17 and he had never had anaphylaxis his whole life either.
His name is Steven and he’s 23 now. We went to a Vietnamese pho restaurant—we’d been eating there for three years or so and my son had always ordered the same dish, but they happened to change the recipe without putting any warning of the change in ingredients. He had a full anaphylactic shock. But we were able to save his life because he had an EpiPen and we were able to get him to the emergency room and get him on IV and get him on a breathing machine.
The other thing is B.J. died at 18; Steven had his first anaphylactic reaction at 17. I tell other people that you might have mild reactions now, but your body changes in time, and once it starts recognizing the allergens quicker, the shutdown of your body can be quicker.
Paul Antico: Can you tell me roughly how many reactions Steven had prior to this anaphylactic reaction, and what his typical symptoms had been?
Brian Hom: Yes. He’s had probably less than 10—because he’s very good at avoiding peanuts. He reads the labels, he will not take a risk, he watches where we eat. He’ll avoid trying anything that’s not labeled or doesn’t know what kind of ingredients are in it.
Paul Antico: Okay, and his reactions in the past, like B.J.’s, had also been relatively mild until this incident?
Brian Hom: Yes.
Paul Antico: Wow.
You said something else when you were talking about the individuals that come into your restaurant and say, “Well, I’ve only had mild reactions.” While we’ll talk about your advocacy in a moment, I’m sure you share some of what you learned with these patrons. How do people react? Do you feel like they believe you more? Are they shocked that this can happen? Or do people usually know but say, “Well, yes, I’ve been told that, but—you know”?
Brian Hom: They’re—most of them are a little bit shocked. Some of them say, “Now I’ll get an EpiPen.” I even talk to the [food-allergic] adults who have young children and say, “You need to carry an EpiPen because it’s tough enough losing a child to food allergies, but [consider] having an adult parent be lost because you chose to take the risk that it’s not going to happen to you? And now your children are motherless or fatherless.”
Paul Antico: Right, that is really important, because there are many adults with food allergies who take them for granted—and especially now, as the first big wave of food allergy kids, as I call them, are in college or coming out of college, and they’re going to be starting families of their own. That’s a great message to give them.
You said you have three boys. What is your other son’s name and does he have food allergies?
Brian Hom: His name is Brandon. What’s interesting about Brandon is, after B.J. had passed, we had him tested. The normal blood test showed that he had a high IgE in his blood [to peanuts], but he’d been eating peanuts all his life. He was 15 when B.J. passed away so we had him carry an EpiPen for a year until he was 16 or almost 17. Eventually, it was determined that that it was safe for Brandon to continue eating peanuts, despite high IgE numbers, so he no longer carries an EpiPen.
Paul Antico: Brian, do you and your wife have allergies?
Brian Hom: Neither my wife, Kathy, or I have food allergies. We do have seasonal allergies, like dust and pollen.
A tree established in memory of B.J. at Chaboya Middle School in San Jose, CA.
Paul Antico: Since B.J.’s passing, you’ve really jumped headfirst into food allergy advocacy, and I’m very thankful for that personally and on behalf of the food allergy community. Could you talk about some of your initiatives and activities?
Brian Hom: After he died, we started a walk for him and did it for five years, to help raise awareness, as part of FAAN (Food Allergy & Anaphylaxis Network, now part of Food Allergy Research & Education). We started it in 2011, I think. I think the first walk I participated in was in San Francisco, because there was no walk in San Jose. I asked FAAN if I could bring one to San Jose, and we did. We raised almost $100,000 a year, which was a lot of money for walks, especially new walks. I also joined FAACT (Food Allergy & Anaphylaxis Connection Team), trying to help raise awareness and raise funds to basically find the cure for food allergies because I don’t want to see anybody else suffer a loss like my family has with B.J.
I’ve been on TV, I’ve been on Lifetime network, I’ve been in newspapers, and I’ve done school assemblies with Kyle Dine, trying to share B.J.’s story. We helped pass legislation, which President Obama signed nationally, that allows EpiPens in schools. It was a voluntary program, so very few schools were doing it because they didn’t want to take on the liability (even though there was no liability). In California, we passed a law that allowed us to mandate it in all public schools in California, so we had Governor Brown sign that petition into law, and then we also recently passed a law to allow EpiPens in restaurants, which I took the lead in California. I put an EpiPen in my restaurant, hoping that by taking the lead, other stores and other restaurants would follow suit.
Paul Antico: That’s fantastic. We’re trying to educate restaurants about their right to carry stock epi [epinephrine autoinjectors] in most states right now, but it’s slow going – this is understandably out of their comfort zone.
I didn’t realize you toured with Kyle Dine. I know Kyle and really respect what he does. Tell me about going to schools with him to help educate young children, especially doing so in a way that doesn’t frighten those who may not be emotionally ready to hear your story.
Brian Hom: I helped set up some of his assemblies in San Jose. We did maybe six, seven, eight assemblies at middle schools and elementary schools.
I would tell my story, being careful not to terrorize the kids, but we tried to tell the story – that it’s serious. It was kind of heartwarming to have a middle school or elementary kid come up and say, “Sorry for your loss,” which is such a compassionate statement from a little kid.
Paul Antico: Yes. How were the reactions of the school administrations themselves, given that there are some schools that really get it and some that have been holding out, for lack of a better way of putting it?
Brian Hom: Well, some of the schools that we did were those that B.J., as well as my other sons, attended, so I knew the principals and I knew a lot of the teachers. They were there with open arms, and you know Kyle, his shows are really entertaining to kids, so it’s a good way to communicate food allergies. We also planted trees there. People saw the trees [that said], “This is in memory of B.J. Hom who died of a peanut allergy”, planted in front of the school. It’s kind of nice—10 years now have passed, and I see these kids, they’re growing up, they’re going to college now, and they say, “Yes, I know—we remember your son’s story, we’ve seen the trees there.”
Paul Antico: Oh, that’s wonderful.
Brian Hom: The community around where I live, San Jose, really embraced it. One of the Emmy-winning newscasters for NBC News also has food allergies – a seafood allergy. She was the emcee for my walk. We also had Kyle at my walk, we had some big entertainers, and we had athletes come and support us.
Paul Antico: One last thing on advocacy. You’re on the Board of FAACT, and you’ve succeeded in getting the school Epi legislation and the public Epi legislation, not to mention everything else we covered. Is there other advocacy that you’re currently involved with? You’ve done so much!
Brian Hom: I opened a restaurant and got involved with Vitality Bowls [restaurant chain] as a franchisee. My involvement now is making a safe place for people with food allergies and also raising awareness. I do that on a daily basis, and that’s what I’m doing now. I’m still on Facebook, involved with a lot of the food allergy community.
Brian and Kathy Hom, who became food allergy advocacy crusaders after their son B.J. died of a peanut allergy reaction, in one of their San Jose Vitality Bowls restaurants. (Photo courtesy of Vitality Bowls)
Paul Antico: Were you interested in the restaurant business before you became a food allergy advocate?
Brian Hom: No.
Paul Antico: Please tell me more about your leap into the restaurant industry.
Brian Hom: The founders of Vitality Bowls, Roy and Tara Gilad, husband and wife, had a four-year-old daughter that had food allergies and could never find a safe place for her to eat. They were into healthy lifestyles and healthy food, so they opened their first store in San Ramon in 2011 and it was successful. They started franchising in 2014.
I was working in the high-tech business for 37 years until 2016. I started looking to work elsewhere when I attended a one-hour seminar on opening your own restaurant franchise. I took the seminar and told them I was into healthy living, and they mentioned, “Oh, there’s this franchise called Vitality Bowls, it’s fairly new, and it was founded by a couple who had a four-year-old who had food allergies. They make sure there’s no cross-contamination, and they have a point of sales that you can label the receipts—food allergy, etc.” I said, “Perfect.” I said, “Here it is, my ability to continue my mission and my advocacy, by raising more awareness and taking the lead that more restaurants will take food allergies more seriously.”
I get a lot of customers who come in and say, “I know you understand how severe food allergies are and how fatal they can be, and I’ve never brought my kids to any restaurant,” and they bring them into my restaurant, which I think is great.
Paul Antico: Wow. Can you tell us a little more about how you keep food-allergic customers safe at your Vitality Bowls restaurant?
Brian Hom: The way we protect people with food allergies is, upon entering the store, when somebody says they don’t want certain ingredients, I ask them if it’s a food allergy or a preference, right at the point of sales. We’re asking customers, “Do you have a food allergy,” basically. If they do, we mark the ticket going to the kitchen, that if they have a peanut allergy, a nut allergy, dairy allergy—or you know, a certain fruit allergy, we make sure we move it to a separate station. We have nut-free blenders, so we can prevent that cross-contamination.
Second, we do have an EpiPen stocked right at the point of sale, to be used on any customer who we see having a severe food allergy reaction.
Third, we have an alarm system in the store that can call the ambulance, can call the fire department across the street, can call the police department, and we can call Kaiser. The Kaiser Emergency Room is within a mile away. I’m willing to drive someone there myself, because I know where it is.
Those are some of the things that we do.
Paul Antico: You’re the first restaurateur I’ve spoken to who carries an epinephrine autoinjector in his restaurant, even though over half the states have laws that allow it. I think that’s fantastic. What was the process of doing it? Was it challenging or easy?
Brian Hom: It was fairly easy. You just need to get a doctor who’s willing to write a prescription for your restaurant.
Paul Antico: But how do they write a prescription if it’s for stock epi?
Brian Hom: When they passed the law in California, I was trying to figure out, “So how do I get it?” Basically, they said just get a doctor to write a prescription, so they write it to me personally.
Paul Antico: Jumping back into your restaurant, what kind of food allergy training does your staff go through?
Brian Hom: We have a certification program that teaches them how to – because we serve peanut butter in the store – how to make what we call a Gladiator sandwich, how to use the red cutting board, move it away from other stations and how to clean up afterward, how to use our nut-free blenders… There’s a full allergy certification checklist that each employee has to sign and get certified.
Paul Antico: Is that from the Corporate parent company, Vitality Bowls?
Brian Hom: Yes, that’s from corporate.
Paul Antico: So it’s not an outside program; it’s Vitality Bowls’ own program.
Brian Hom: Yes.
Paul Antico: Oh, that’s great. Now, if I had a group of restaurateurs in front of us and asked you, “What’s your best advice for them,” what would you say?
Brian Hom: To make sure your staff understands how severe food allergies can be, and that you really need to take food allergies seriously. At the restaurant where Steven had his anaphylactic reaction, where they didn’t label the allergen, the management told me that they were going to label their menus, and it’s now been six years and they’ve [still] done nothing. Don’t wait until you get a lawsuit [or worse!], to have to change your thoughts on food allergies.
Paul Antico: Do you feel like a lot of restaurants by you “get it” with respect to food allergies?
Brian Hom: Nope. Only the big chains that actually have programs, have food allergy training, menu guides, and stuff.
Paul Antico: You think that there needs to be a lot more education, particularly with the independents, and a lot more training?
Brian Hom: Correct.
Paul Antico: I know this is not about the money for you, but do you find there are financial benefits to having a restaurant that’s allergy-friendly versus otherwise?
Brian Hom: Yes, because I find that probably 25% of my customers have food allergies.
Paul Antico: Wow, and I assume they become your more regular customers?
Brian Hom: Yes, we have a lot of them. Gluten intolerances, people with nut allergies, dairy allergies, some fruit allergies. Some people have strawberry allergies or such, but yes. It’s just amazing.
Paul Antico: Before my last question, I again want to thank you for all your support of the food allergy community and once more offer my sympathies for how it began. Hopefully your efforts over all these years has helped saved the lives of other children and adults. My guess is that they have.
So finally, are there any other key takeaways from this long journey you’ve had that you would share with either the food allergy community, restaurateurs, other advocates or the general public? Anything big that we haven’t talked about?
Brian Hom:Yes. I would just give this advice. Losing a child is very difficult. Losing them to food allergies is just mindboggling.
If you have an opportunity to make it safe as a restaurateur, or make it safe as a parent, or anything, help people understand that food allergies can be fatal. You only get one chance. You don’t get a second chance.
The day that B.J. died, I thought it was a bad dream and that I would wake up, and that he would wake up and I would get a second chance. But my takeaway for everybody is to take food allergies seriously. It can become fatal, and you need to do everything you can, and don’t let your guard down. Be vigilant to prevent having a fatal reaction to food allergies.
Anything people can do that helps support finding a cure or finding the cause of food allergies so that we can reduce the numbers—and from a restaurateur’s point of view, if we don’t find out why food allergies are on the rise and how to cure it, restaurateurs are going to be impacted. People are going to stop eating out. They’re going to have to start eating at home and really doing things to protect themselves. We as restaurateurs—everybody’s going to have food allergies soon and if you don’t start making the changes now – I don’t think the restaurateurs who don’t take food allergies seriously will be around very long.
Paul Antico: Yes. Well, thank you, Brian. I’ll tell you, as a parent, and not having gone through what you have, it’s at times really difficult to listen to your story – and I really appreciate you being willing to share it with us. I can only imagine that it’s painful every time you do it, so again thank you so much.
Once again, I can’t express my appreciation enough to Brian for sharing his story and for all he has done, and continues to do, as an allergy superhero in our community.
Personally, I’m making sure to have my children read this story. I confess that this was a big wakeup call, even to me, about the risks of what we mischaracterize as “mild” food allergies. Sure, I’ve heard doctors say again and again that the severity of one reaction does not indicate anything about the severity of future reactions, but “our situation was different.” With particular allergens, my kids “only have mild reactions,” easily treated with Benadryl. Certainly, we’ve never let them eat without an AUVI-Q (epinephrine autoinjector), but I guess it’s fair to say that I’ve felt pretty comfortable that nothing truly bad would happen when the inevitable mistake occurs again.
No longer. I need to be as serious and vigilant about the real risks from each of their allergens now as I was after the initial diagnoses. More importantly, I need to set that example and teach my kids even more firmly to never take their allergies for granted as they go off into this world on their own, which they’re now doing.
I thank Brian for that important reminder. I can only wonder if any lives have already been saved by the sharing of his story and his advocacy efforts over the past 10 years.
I also appreciate Brian taking the lead in keeping epinephrine autoinjectors in his restaurant. I doubt even 1% of restaurants in the states that allow “stock epi” know about it. This is another element we need to share. I know many restaurants in my home state of Massachusetts (where stock epi is not yet allowed in restaurants) are ready and willing to take advantage of this opportunity to provide another layer of protection for their guests.
I’m sure Brian’s story has touched many of you who have read it in different ways. Please share any thoughts or comments here. We want to hear your voices.
Also, if anyone has had a chance to visit Brian’s Vitality Bowls restaurants in San Jose, please review your experience on AllergyEats’ restaurant pages. In fact, we’d love to see more reviews of all Vitality Bowls restaurants, as this is a relatively new, growing chain that seems to have a lot of promise for our community nationwide. (Of course, we still encourage reviews of every dining experience you have every time for the benefit of all of us.) We’re all in this together!
A stock epinephrine and mandatory food allergy education program for the hospitality industry in the City of Toronto is the right thing to do. It has huge benefits for the safety of the general public and increases public awareness of food allergies.
This week I had the honour of providing a public deputation for Toronto City Council alongside Food Allergy Canada in support of Councillor James Pasternak’s motion to investigate mandatory stock epinephrine at Toronto restaurants. The summary of the motion states:
Given that the City of Toronto is home to over 8,000 restaurants and hundreds other public facilities, it is worthwhile to investigate if the mandatory provision for epinephrine auto-injectors in restaurants and public facilities would enhance the safety of residents and visitors to our City.
Going into it, I knew we were facing an uphill battle with the idea of mandatory epinephrine, but the motion was to investigate the issue. My optimism (and naivete) led me to believe that the investigation could lead to discussions with various stakeholders across the city, and whether or not the mandatory stock epinephrine motion would be eventually tabled, food allergies would be discussed as a growing public health concern.
I am utterly disappointed that the Licensing and Standards Committee voted to “defer indefinitely” the motion to investigate mandatory epinephrine in Toronto eateries and other public facilities. The conversation ended before it even begun.
The councillors seemed to be making advance judgement based on personal bias on the appetite for mandatory stock epinephrine in Toronto restaurants, and not interested in undergoing at true investigation. Unfortunately, the supporting document for the motion was a simple one-pager that did not contain many supporting facts to help push this forward. Despite the huge outpouring of public support letters in favour of the motion, there were two very strongly opposed positions coming from the hospitality industry, which councillors seemed to give more weight to. It’s obvious that if a motion like this has any chance to move forward in the future, there needs to be a champion from the industry backing it and explaining why it makes sense operationally.
The most important takeaway from this experience is that, as a community, we haven’t even scratched the surface when it comes to educating the public about food allergies and epinephrine. The city councillor comments and the information they used to come to their final decision were based on assumptions, miseducated testimony and untruths. I am compelled to set the record straight.
Untruth #1: Epinephrine is not the only appropriate drug to use in an allergic reaction
Councilor Jim Karygiannis stated, “I have severe allergies. I choose not to use an EpiPen and I choose to use Atarax. Atarax might not have the same effect immediately, but it’s a slower process, because I choose not to go to the hospital if I shoot myself with an EpiPen in 20 minutes, because I might not be able to get there.”
Antihistamines like Benadryl or Atarax are commonly used for treating hives or other skin symptoms, but they do not treat the life‑threatening symptoms of anaphylaxis. “Epinephrine is the only drug that can reverse symptoms of anaphylaxis. Canadian allergists advise that an epinephrine auto-injector is the first line of treatment for anaphylaxis and should be used first, before asthma puffers or any other medications,” according to Food Allergy Canada.
An EpiPen is actually much easier to use than some may realize.
Epinephrine acts on a number of receptors in the body to exert its effects. It causes constriction, or tightening, of the blood vessels, which decreases swelling and also helps to increase blood pressure. It also increases the heart’s contraction and heart rate, which can help to prevent or reverse cardiovascular collapse. Epinephrine relaxes the muscles around the airways in the lungs, helping the airways to open up. Finally, it prevents the release of additional allergic chemicals, which aids in stopping further progression of the reaction. No other medicine acts on so many body systems, which is why epinephrine is the drug of choice for anaphylaxis.
Untruth #2: EpiPens could cause fatal harm
Councillor Jim Karygiannis asked, “So, this could have a reverse effect that somebody thinks they’re having an allergic reaction, hits somebody, and that might cause them fatal harm?” Commander Bikram Chawla with Toronto Paramedic Services responded, “Theoretically, there is that potential.”
Common side-effects of epinephrine include fast, irregular or “pounding” heartbeat, sweating, nausea or vomiting, breathing problems, paleness, dizziness, weakness, shakiness, headache, feelings of over excitement, nervousness or anxiety. These side-effects usually go away quickly if you lie down and rest.
The minimum lethal human dose by subcutaneous injection is estimated at 4mg. EpiPens come in two standard doses of 0.15mg and 0.3mg of epinephrine, which is significantly lower than a dangerous dose. To put things into perspective, you would need 26 simultaneous shots from an EpiPen Jr. to receive a dangerous dose.
Untruth #3: Food allergy and auto-injector training is too difficult
Councilor Frances Nunziata shared, “I do have an EpiPen. I have allergies. I’ve had to use mine many times. But I would not feel comfortable being in a restaurant or any establishment and having someone stab me with an EpiPen not knowing how long they’ve had that EpiPen… So to have establishments and restaurants like Tim Horton’s and McDonald’s be trained, I think we’re in really muddy waters.”
An EpiPen is actually much easier to use than some may realize. The instructions are illustrated on the device in three simple steps. Practice EpiPens also help make training easier and more effective.
It has huge benefits for the safety of the general public and increases public awareness of food allergies.
Assumptions that every single staff member in the restaurant would need to be educated like a paramedic so they could recognize symptoms of allergic reactions and administer EpiPens made this motion difficult for council to support. They did not recognize that like AEDs that are available at public places, EpiPens would be available as life-saving devices to the people who need them and know how to use them.
A stock epinephrine and mandatory food allergy education program for the hospitality industry in the City of Toronto is the right thing to do. It has huge benefits for the safety of the general public and increases public awareness of food allergies. Restaurant staff are currently trained at different capacities on how to keep customers safe by minimizing risks of bacterial food poisoning, and it is equally as important that they are trained on food allergies and how to minimize cross-contamination risks.
There is still a lot of work to be done. As a food allergy advocate and someone invested in the City of Toronto, I’m grateful to Councillor Pasternak for bringing the motion forward and to the Licensing and Standards Committee for discussing the possibility. As a community we will move onwards and upwards from this and continue to educate others and correct untruths.
(Reuters Health) – If restaurants and other food establishments stocked epinephrine autoinjectors, the number of fatal allergic reactions, known as anaphylaxis, could decrease, a small study in Canada suggests.
After a two-year test of an epinephrine autoinjector stocking program in Hamilton, Ontario, diners with allergies as well as restaurant owners and staff said that having the devices onsite made them feel better about possible emergencies, researchers report in The Journal of Allergy and Clinical Immunology: In Practice.
The costs varied by how many staff needed to be trained to use the devices, but the expense was low compared with that of automated external defibrillator (AED) devices, the study authors note.
“Self-management of food allergy and anaphylaxis is sub-optimal, particularly among adolescents and young adults who most often engage in risk-taking behaviors such as neglecting to carry epinephrine autoinjectors or delaying its timely administration to treat reactions,” said lead author Dr. Susan Waserman, a professor of medicine at McMaster University in Hamilton and director of the Adverse Reactions Clinic at the Firestone Institute of Respiratory Health.
Between 1986 and 2011, about half of anaphylaxis deaths in Ontario were due to food allergies, and 14 percent occurred after eating at restaurants, fast food chains or shopping mall food courts.
In the U.S., more than half of anaphylaxis deaths occur at restaurants or other food establishments such as ice cream shops and food courts, the study team writes.
“Challenges also exist in food establishments, including the lack of knowledge and training of food service personnel about food allergies and the reluctance of food-allergic individuals to disclose their allergies to restaurant staff due to embarrassment,” Waserman told Reuters Health by email.
To test the feasibility of stocking epinephrine injectors in places where severe allergic reactions to food might occur, the researchers implemented a program at a Hamilton shopping mall between 2014 and 2016. Security guards had access to autoinjectors in first aid kits in the mall’s central administration office and received training on recognizing allergic reactions and how to use the injectors.
In two mall restaurants, staff were also given the three-hour training session and had access to injectors kept in a central area, such as behind the counter, as well as back-up doses kept in an office area. Each location also had a site leader and an anaphylaxis emergency response plan.
Only one critical incident occurred during the study period, so it is difficult to show the full benefits of the program, the study team writes.
However, since the pilot program, government-owned properties in Hamilton such as recreation centers, arenas, senior centers and community halls have installed autoinjectors. After finding that firefighters often arrive on the scene for anaphylaxis emergencies before ambulances, the Hamilton Fire Department also stocked its fire trucks with autoinjectors. The program is now in 50 restaurants across the city, with the goal of reaching all 2,000 restaurants in Hamilton.
The success of the epinephrine autoinjector stocking program depends on several factors, including local government support, effective staff training, low resource requirements and embedding the program into existing policies and procedures, Waserman’s team writes.
Costs in the pilot program ranged from C$715 ($543.93) for the sit-down restaurants to C$2,155 ($1,639.41) for the mall-wide program, they note.
“Whether you’re diagnosed with an allergen already or have your first allergic reaction at a restaurant, this could stop a potentially life-threatening moment,” said Dr. Scott Sicherer of the Icahn School of Medicine at Mount Sinai in New York City, who was not involved in the study.
“When you eat outside of your home, you depend on other people to make food for you,” he said in a phone interview. “This program is a good model that makes sense.”
Legislation and liability issues may pose more of a problem in the U.S., he added, since epinephrine autoinjectors are typically only available by prescription. Now that some schools are beginning to carry them, however, that could open the door for other public places.
“At a restaurant, you can say you have an allergy and you can carry a card with instructions,” Sicherer said. “A chef or server may guarantee they can provide a safe meal, but when that means just scraping nuts off the top of a salad, that doesn’t work, and you may not realize.”
SOURCE: bit.ly/2nEwQIW The Journal of Allergy and Clinical Immunology: In Practice, online August 2, 2018.
ANNAPOLIS — A bill allowing certain food-service operations to administer auto-injectable epinephrine, or EpiPens, in an emergency breezed through the General Assembly this week as the abbreviated session expired.
After a tragedy last October that claimed the life of a popular local man and business owner, some questioned if the outcome could have been different if restaurants and other food-service operations were allowed to obtain, store and utilize EpiPens and had certain staff trained and available to utilize them in the case of an emergency. Maryland is currently one of just 14 states that does not allow most food-service operations to obtain, store and utilize EpiPens.
Urged by resort officials, State Senator Mary Beth Carozza introduced Senate Bill 477, which would “authorize food service facilities to store and make available for administration auto-injectable epinephrine for a certain purpose under the program, authorize participating food service facilities, except under certain circumstances, to obtain a certain prescription for and supply of auto-injectable epinephrine, and require participating food service facilities to store a supply of auto-injectable epinephrine in a certain manner.”
Over in the House, Delegate Wayne Hartman (R-38C), along with other state delegates, introduced sister legislation House Bill 1462. Both bills passed unanimously in their respective chambers and crossed over where they were returned passed by both the Senate and the House.
The full Senate passed the legislation with a 47-0 vote on Monday and the full House followed suit with a 130-0 vote on Wednesday as the General Assembly session abbreviated by concerns over the ongoing coronavirus pandemic neared its close. The legislation is now headed to Gov. Larry Hogan’s desk for signing and will become effective on Oct. 1.
The bill requires eligible food service institutions to obtain a certificate allowing it to obtain, store and administer auto-injectable epinephrine in an emergency situation. The certificate holder would designate certain eligible agents certified in administering the EpiPens. For example, the agents would have to be at least 18 years of age and would have to successfully complete an educational training program.
Under the legislation, the participating facilities will designate the employees who are certificate holders who will be responsible for the storage, maintenance and control of the supply or auto-injectable epinephrine.
A participating facility would not be able obtain or store auto-injectable epinephrine unless it has at least two employees or designated affiliated individuals who are certificate holders. Participation in the epi-pen program would be strictly voluntary. In addition, provisions in the bill would provide immunity from liability under the state’s Good Samaritan laws.
In late October, local resident and pillar of the community Chris Trimper suffered an extreme allergic reaction during a reception at a local food service facility and did not survive. In the wake of the tragedy, local elected officials and resort business leaders called on their delegation in Annapolis to introduce legislation that would allow certain food service operations under certain specified conditions to store and administer epinephrine in the event of an emergency.







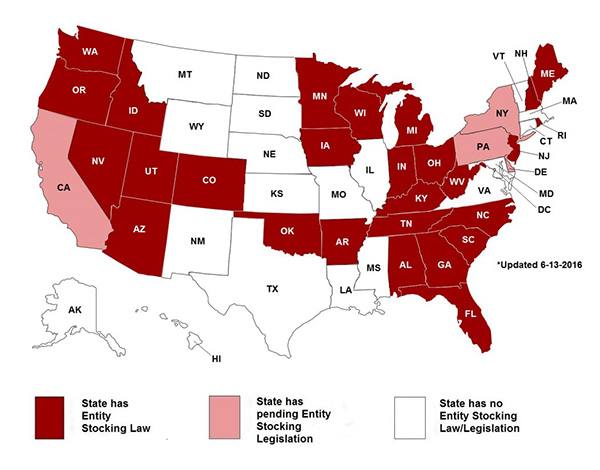



 Kaléo, which manufactures a competitor auto-injector, Auvi-Q, has no such availability concerns. “Kaléo has not been impacted by the supply issues reported by other epinephrine auto-injector manufacturers,” said Caryn Foster Durham, director of corporate communications at Kaléo.
Kaléo, which manufactures a competitor auto-injector, Auvi-Q, has no such availability concerns. “Kaléo has not been impacted by the supply issues reported by other epinephrine auto-injector manufacturers,” said Caryn Foster Durham, director of corporate communications at Kaléo.
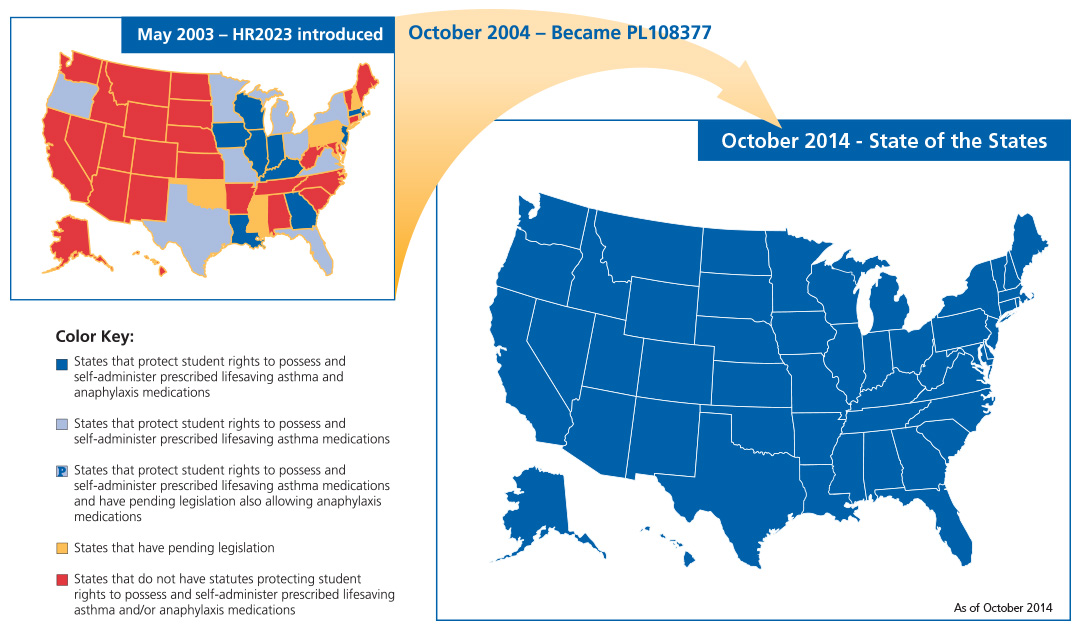




 Would I avoid talking about what happened to my child and food allergies in general? Or would I have the courage, strength, and drive to dive deeper into the food allergy world in an effort to save others from facing similar devastation?
Would I avoid talking about what happened to my child and food allergies in general? Or would I have the courage, strength, and drive to dive deeper into the food allergy world in an effort to save others from facing similar devastation?






